Stages of Pressure Injuries: For Hospital Staff
Evaluating pressure injuries includes describing and documenting them and tracking their progress. Keep in mind that many patients who are prone to developing pressure injuries may have a decreased ability to sense pain or discomfort. Staging systems provide you with a guide in this evaluation process. According to the National Pressure Injury Advisory Panel (NPIAP), staging does not refer to a step-wise sequence in either direction (progression or regression). NPIAP does not recommend the practice of reverse staging, or changing the stage as healing occurs. The information in this sheet is an overview of the staging and treatment of pressure injuries. Always follow your facility’s specific guidelines.
Remember to Assess, Describe, and Document.
Deep tissue pressure injury
The unbroken skin is deep red, purple, or maroon and looks bruised. Or there is a blood-filled blister. The area is painful, firm, mushy, boggy, warm, or cool to the touch. The cause of this skin change is pressure and/or shear, injuring the underlying soft tissue. The skin change could heal or progress to more severe stages of pressure injury.
Goal: Determine the extent of the injury, support blood flow, and prevent further breakdown of skin.
-
Redistribute pressure. Set up a schedule to reposition patient.
-
Obtain a pressure-reducing support surface such as static foam, dynamic pressure, or air-filled mattress to decrease pressure.
-
Prevent shear, friction, and moisture buildup.
-
Reassess the patient.
-
Assess and manage the patient's pain of injury.
-
Assess for infection.
-
Discuss pressure injury with the healthcare provider.
Stage 1 pressure injury
The unbroken skin is red and nonblanchable. Note: It may be difficult to determine blanching in darker skin tones. The affected area may differ in color from the surrounding skin. In this case, pay particular attention to changes in skin temperature, edema, sensation, and any difference in tissue consistency compared with surrounding tissue, like firmness.
Goal: Prevent further progression of the injury and support blood flow.
-
Implement treatment plan for deep tissue pressure injury.
-
Keep the skin clean and dry. Use a pH-balanced agent for cleansing. Don't use hot water for bathing.
-
Lightly moisturize the skin. Note: Never massage the affected area. This can cause further damage to tissue. Allow the moisturizer to dry before placing any additional pressure on the area.
-
Apply protective dressing, if indicated.
-
Encourage mobility, as tolerated.
-
Evaluate nutritional intake.
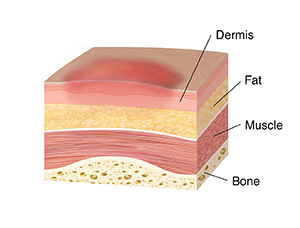
Stage 2 pressure injury
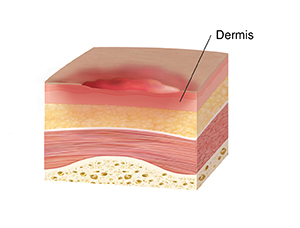
Partial-thickness skin loss has occurred with the dermis exposed. The wound bed is viable, red-pink in color, and moist. Slough, granulation tissue, or eschar is not present, but a broken or intact serum-filled blister may be evident.
Goal: Prevent full-thickness injury and continue to promote healing.
-
Implement treatment plan as for previous stages.
-
Apply dressing to keep wound bed moist and promote healing.
-
Protect fragile skin from adhesives and irritants.
-
Reevaluate nutritional intake.
Stage 3 pressure injury
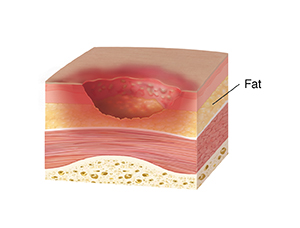
Full-thickness skin loss has occurred. Slough and eschar may be present. Subcutaneous fat may be visible, but bone, tendon, or muscle are not. Undermining or tunneling may also be present.
Goal: Maintain a clean, moist wound bed to prevent infection and promote new tissue growth (granulation).
-
Implement treatment plans as for previous stages.
-
Remove dead tissue (debridement) if needed.
-
Absorb drainage.
-
Fill the injury cavity with an appropriate dressing.
-
Optimize protein and total calorie intake based on nutritional consultation.
Stage 4 pressure injury
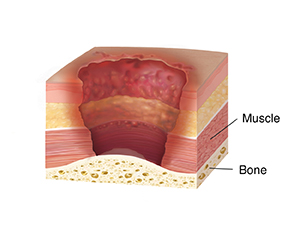
Full-thickness skin loss has occurred. Bone, tendon, or muscle is exposed. Slough or eschar may be present, but the base of the wound can be seen. Rolled edges, undermining, and tunneling are often present.
Goal: Reduce drainage, remove dead tissue, and establish an environment for new tissue growth.
-
Implement treatment plans as for previous stages.
-
Report bone involvement.
-
Treat infection with antibiotics, if indicated.
-
Discuss with the healthcare provider whether surgery is needed.
Unstageable full-thickness pressure injury
Full-thickness skin loss has occurred. Slough or eschar covers the wound base. The wound depth can't be determined because of the slough or eschar.
Goal: Determine stage, provide moist environment, and prevent further breakdown.
-
Debride the wound. Don't debride dry, adherent, intact eschar on the heel unless signs of infection are present.
-
Reassess pressure injury stage once base is visible.
-
Manage pain of injury.
-
Assess for infection.
-
Discuss pressure injury with the healthcare provider.